

Rib Pain
Rib pain is a common reason to visit your Chiropractor. The most common place for rib pain to occur is in the back right next to the spine. Pain can also occur throughout the rib cage. It is also quite common for rib pain to develop in the front of the chest at the sternum. Although rib pain is not usually a sign of serious underlying pathology, it certainly can be. Because any chest pain can be associated with heart or lung problems, it is best not to take chances. Get cleared for serious pathology first. In the case that your pain is a musculoskeletal issue, then your next call should be to a Chiropractor.
Musculoskeletal Causes of Rib Pain
Pain in the chest or ribs is a fairly vague complaint. Identifying exactly where the pain is located can be very helpful. Generally, Ribs are designed to move up and down so that your rib cage can expand and contract so you can breath. For this reason many people with rib dysfunction feel as if they are having trouble with their lungs even when the problem is musculoskeletal. Rib Pain is often related to the muscles and joints of the rib cage. Additionally nerves, rib cartilage, and even the bones themselves can be the culprit.
Anatomy Behind Rib Pain
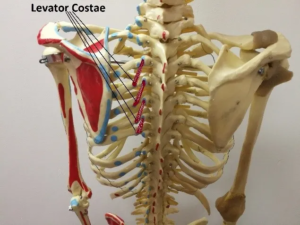
First off, let’s talk a little anatomy. The ribs begin at their attachment to the spine and wrap around the body. At the front of the body, the ribs stop being bones and actually become cartilage before they connect to the sternum. This is so that the rib cage can be flexible and provide mobility to the body and also to aid in breathing. Strong fibers connect the cartilage to the sternum. The key muscles are the intercostals and the levator costae. The intercostals run between the ribs providing stability and pull the ribs together during exhalation. The levator costae attach from the vertebra to the back part of the ribs and lift the ribs during inhalation. Intercostal nerves exit the spine and run between the ribs along side the veins and arteries.
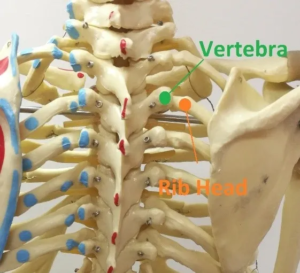
Rib Head Misalignment
This is a very common scenario where the connection of the rib and spine moves out of place. For this reason, it is often called a “rib out”. It can happen during a wrong movement like a sneeze while turned. Patients often describe it as point pain right next to the spine accompanied by radiating pain into the back. Pain is worse upon inhalation, chiefly at the top of the breath. If it is severe, pain can wrap around the rib cage or even feel like there is a knife-like pain going through the chest. Often, patients land in the hospital thinking that they are having a heart attack. Once the doctors rule out any serious heart or lung problems, they usually diagnose a muscle spasm and discharge. Afterwards, patients remain with severe pain until the rib head is “set” by a Chiropractor.
Intercostal Myalgia
This is essentially a pain and spasm in the muscles between the ribs. Reasons can range from trauma to simply sleeping in a bad position. Pain is usually felt to wrap around the side of the rib cage. Postural abnormalities like scoliosis or any deviation of the thoracic spine can be an underlying cause. In fact, the solution often involves improving posture with Chiropractic and physical therapy. Therapies like muscle scraping, massage, electro-stimulation, and ultrasound are also particularly useful.
Intercostal Neuritis
Neuritis means inflammation/irritation of the nerves. Any pressure on the intercostal nerves can produce a shooting, burning, or electric sensation between the ribs. Causes range from spinal and rib misalignment to space occupying lesions along the nerves path. Most commonly, the culprit is a pinched nerve in the thoracic spine. Correction with Chiropractic manipulation usually resolves the issue. Though, underlying postural distortions need be addressed. Additionally, it is possible that shingles (a resurgence of chicken pox) can be responsible for irritation of these nerves. Therefore the skin should be assessed for a rash in the affected region.
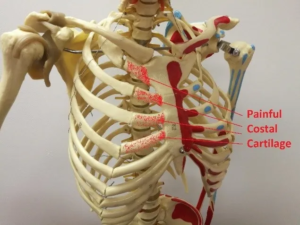
CostoChondritis
Costochondritis is inflammation and irritation of the connection at the rib cartilage and sternum. Pain is typically felt just to the side of the sternum. One or both sides can be affected. The problem usually lies in the connective fibers between the rib and sternum. An alteration of the shape of the rib cage can create stress at this location. The underlying cause is typically postural. Although the problem occurs at the rib, manipulating the connection between the sternum and rib should be avoided. Once the area is inflammed, it is not very tolerant of any more movement. Therefore, manipulation of the thoracic spine and other areas of the cage to normalize the positioning of the ribs is a much better approach.
Rib Strain
The associated muscles surrounding the ribs can become damaged just like any other muscle. Intercostal muscles are usually the culprit, but the levator costae are also prone to damage. Other muscles like the rhomboids or serratus anterior can also be damaged and cause rib pain. Rest and specific stretching is usually fairly effective. Other modalities like E-stim can be effective, but should only be applied by an expert as to avoid current through the heart.
Rib Sprain
Although it is something of a misnomer, a rib sprain is commonly diagnosed to indicate damage done to the costal cartilage. Being that there isn’t actually a bone in the front part of the ribs, it cannot be called a fracture. Costal cartilage is more flexible than the bone, but also more prone to damage. The rib cartilage will heal on it’s own, but getting adjusted and doing some specific stretches and exercises can help.
Rib Fracture
The boney part of the rib cage can be fractured during trauma. Often, there is nothing much to be done besides allow this to heal. If the fracture results in displaced bone or puncture, this is a more serious situation requiring hospitalization and surgery. For less severe fractures there are a few things than can be done such as taping, rehab and ultrasound. Taking regular breaths will also help to prevent the lungs from collapse or resorption.
Treatment for Rib Pain
For non-emergency rib issues, there is quite a bit that can be helpful. Of course the treatment depends on the diagnosis such as above. However, typical treatment for rib pain includes some of the following:
- Manipulation of the spine and ribs
- Soft Tissue Manipulation (like scraping)
- Rehab: Stretches and exercises to improve mobility and posture
- Ultrasound to help with healing and inflammation
- E-Stim to help with pain and spasm
What To Do If You Have Rib Pain
First consider that this may be an emergency situation. Signs of an emergency include: pressure on the chest (like an elephant is sitting on your chest); shortness of breath, feeling faint, a bad cough or flu-like symptoms; pain that spreads to your jaw or arm; dizziness; excessive sweating, nausea, or fast heartbeat. If you have these symptoms, it is best to call 911 or get to the hospital. In the case that you have already been cleared by your doctor, then your next step is to contact a Chiropractor. If you are in the Tulsa area, give us a call. You can even request a free consult by clicking below.