
Shoulder Arm and Hand Pain
Below is a description of most common conditions for Shoulder, Arm, or Hand Pain. While I hope this info helps to provide some insight, it is not a substitute for a doctor’s visit. There are some other very serious reasons behind pain that may require immediate medical attention, so please don’t take the risk of self-diagnosing. Please see a physician like a Chiropractor who can differentiate between a musculoskeletal cause of your pain, and other more serious conditions.
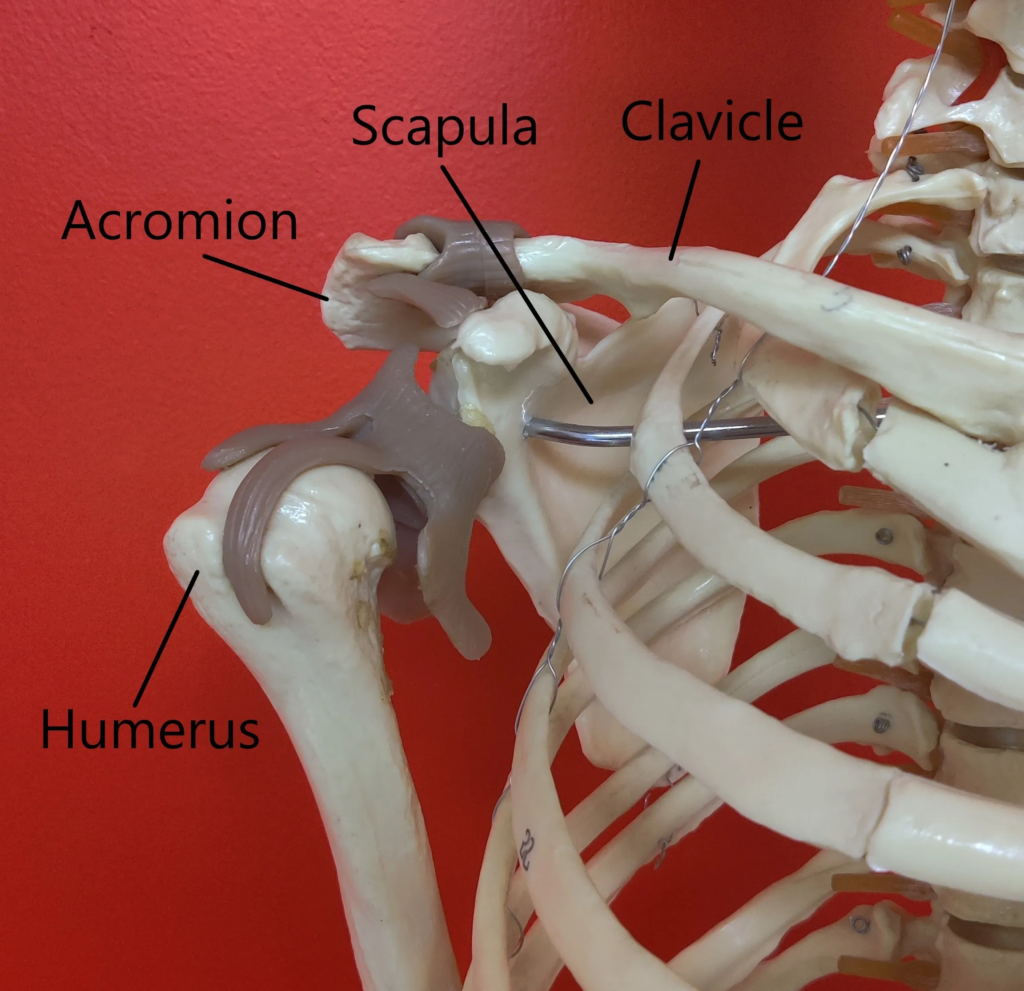


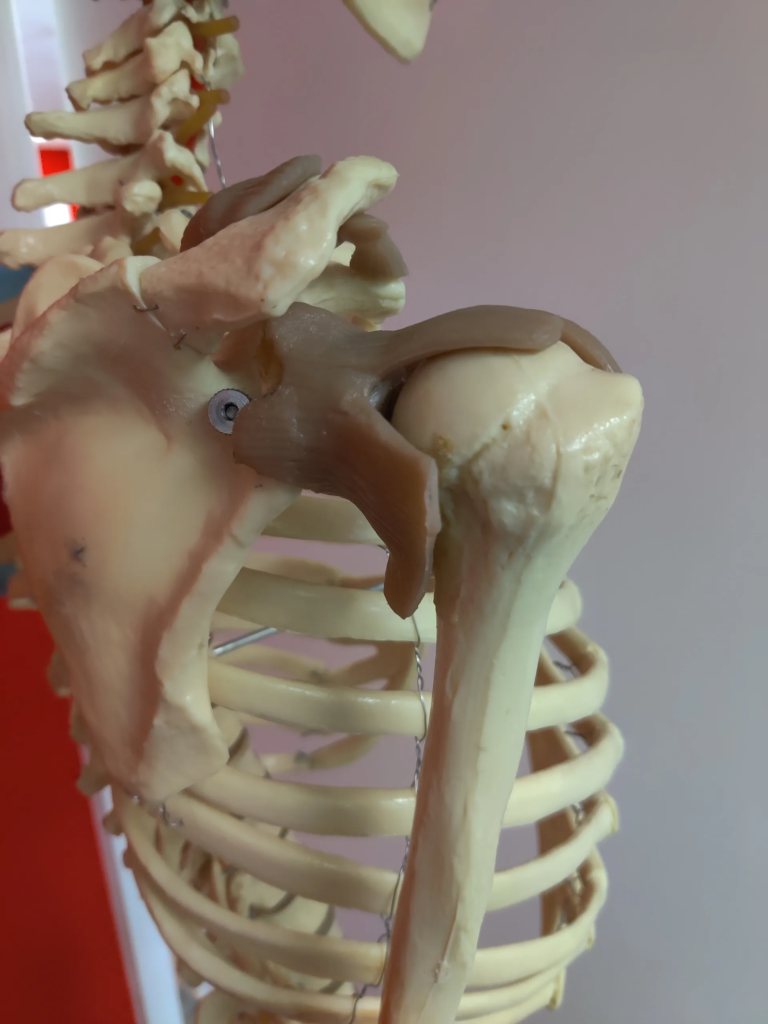
Shoulder Pain
Click above for further detail about shoulder pain causes and diagnosis. The section includes explanation of causes and treatments for each item below. Additionally, don’t forget that you can book a free consult with us by clicking the form link at bottom of the page.
- Acromio-Clavicular (A/C) Joint
- Rotator Cuff Pathology
- Subacromial Bursitis
- Shoulder Impingement
- Shoulder Tendinopathies
- Shoulder Strains
- Glenohumeral Arthritis
- Frozen Shoulder
- Labral Tear
- Referral Pain
- Radiating pain
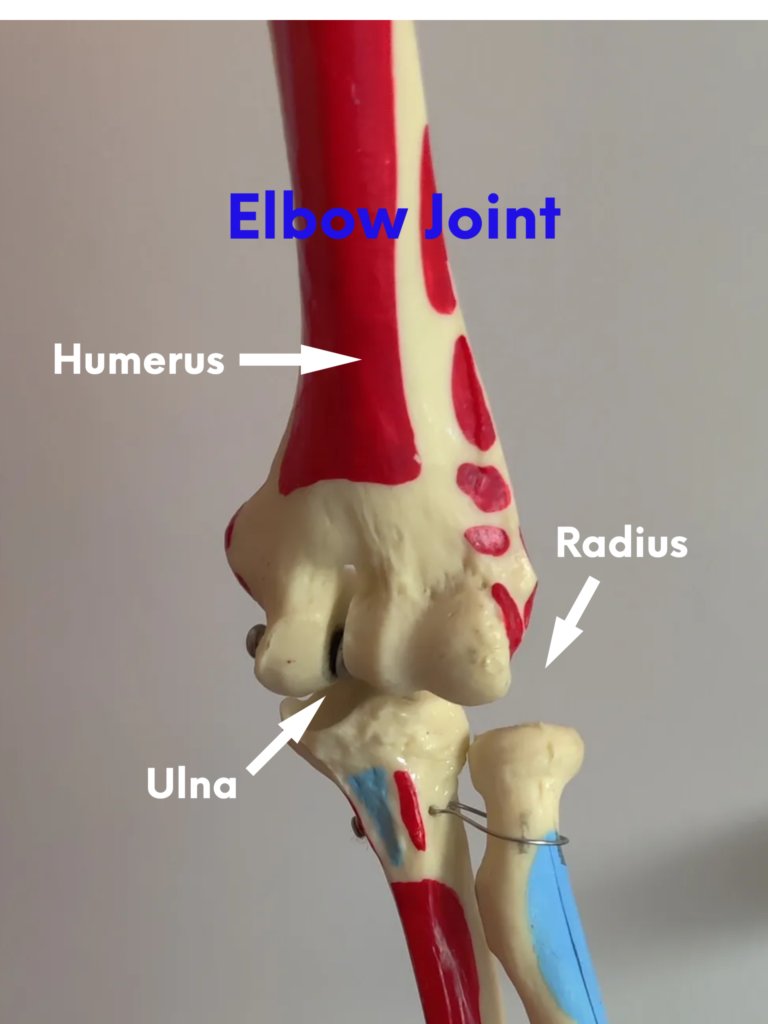


Elbow & Arm Pain
Click above for further detail about Elbow and Arm pain causes and diagnosis. The section includes explanation of causes and treatments for each item below. Additionally, don’t forget that you can book a free consult with us by clicking the form link at bottom of the page.
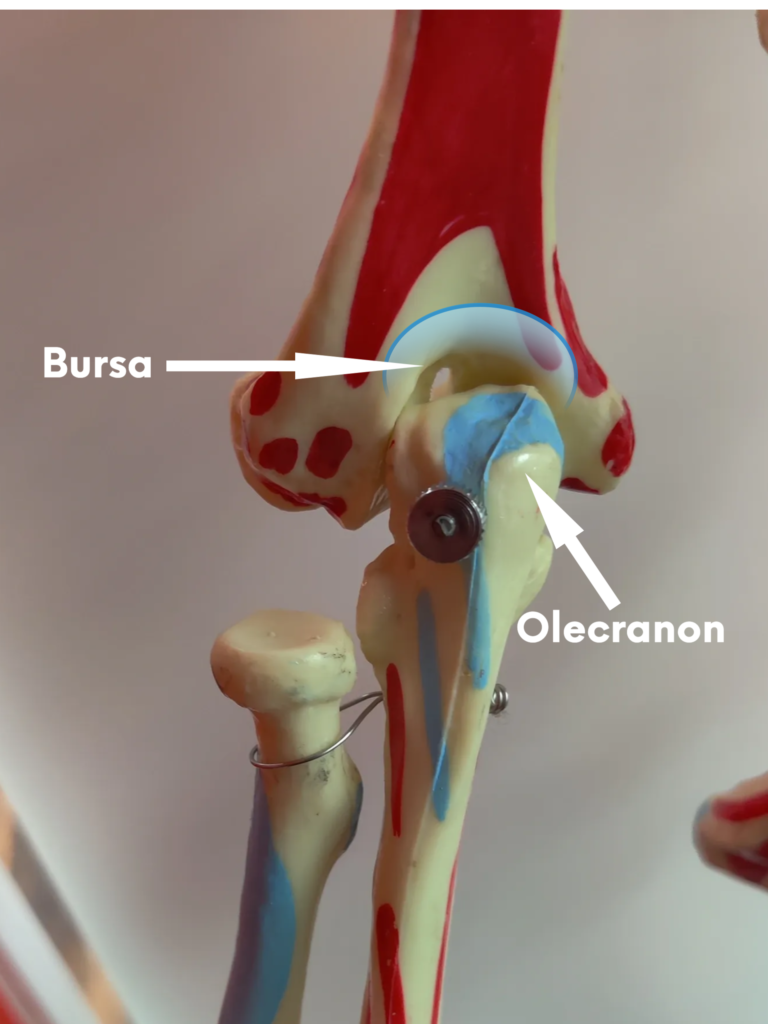
- Arthritis & Olecranon Bursitis
- Tendinopathies
- Tennis Elbow
- Golfer’s Elbow
- Cubital Tunnel Syndrome

Wrist, Hand, & Finger Pain
Click above for further detail about Wrist, Hand, and Finger pain causes and diagnosis. The section includes explanation of causes and treatments for each item below. Additionally, don’t forget that you can book a free consult with us by clicking the form link at bottom of the page.
- Carpal Tunnel Syndrome
- Ulnar Tunnel Syndrome
- De Quervain’s Tenosynovitis
- Ganglion Cysts
- Sprains and Strains
- Elbow Arthritis
- Trigger Finger
What to do if you have Shoulder Arm or Hand Pain
Feel free to give us a call if you have questions or request a free consult on from this website.
Note that NERVE PAIN is addressed in a different section here.